Speak-Up Culture: How the Leader's Noticing Scales
Speak-up culture is the team-level behavioral pattern in which members raise concerns, errors, near-misses, and unmet needs to people with more authority, without waiting for permission. It is not the same thing as psychological safety; psychological safety is the precondition, speak-up culture is the observable behavior that emerges when the precondition holds.
A single leader can notice only what one person can notice. A team in a healthcare unit produces signals at a rate no individual can absorb. The mechanism by which the team makes itself visible to the leader, beyond what the leader can personally observe, is speak-up culture.
Speak-up culture is the team-level behavioral pattern in which members raise concerns, errors, near-misses, disagreements, and unmet needs to people with more authority, without waiting for permission. It is the empirical anchor of Component 1 (Notice) at the team scale and depends on Component 2 (Interpret) for its survival. A team that experiences punitive interpretation when it speaks up will speak up once, learn the lesson, and stop. Speak-up culture is therefore not a separate intervention; it is what Components 1 and 2 produce together when both are working.
In healthcare, the stakes of this scaling mechanism are unique. Patient safety depends on the surfacing of near-misses, the reporting of errors, the willingness to challenge a senior colleague's plan when something is off. The clinical evidence base on speak-up failures (sentinel events, never events, retained foreign objects, wrong-site procedures) is reliably traceable, after the fact, to a culture where someone saw what was about to go wrong and could not bring it forward.
The Construct Defined
Speak-up culture is sometimes treated as interchangeable with psychological safety. The two are tightly linked but operationally distinct. Edmondson (1999, 2018) defines psychological safety as the team-level belief that one can take interpersonal risks (admit error, ask a question, challenge a senior colleague) without facing humiliation, punishment, or career penalty. This is a belief about the team. Speak-up culture is what people actually do when the belief is in place: they raise the concern, report the near-miss, name the disagreement.
The distinction matters because organizations sometimes claim psychological safety based on survey data while still failing at speak-up. Belief without behavior is incomplete; behavior is the diagnostic that confirms the belief is operational. A leader who wants to know whether psychological safety exists on their team should not ask whether people feel safe. They should look at whether people are bringing forward what is hard to bring forward.
The Speak-Up Diagnostic: Is It Safe? Is It Worth It?
Stephen Sledjeski's two-question matrix cuts through the complexity. When team members decide whether to speak up, they are implicitly answering two questions: Is it safe to say this? and Is it worth it—will anything actually change? The combination of answers produces four organizational states.
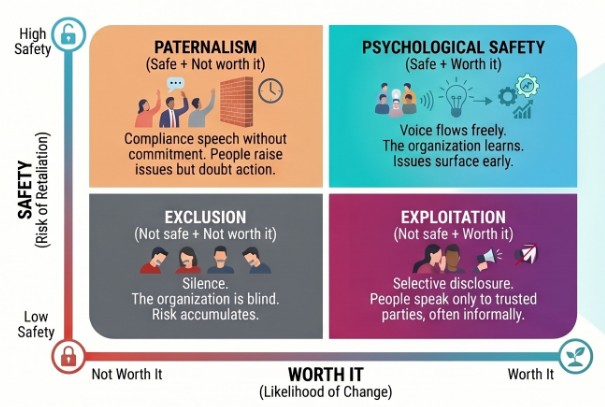
Psychological Safety (Safe + Worth it, upper-right): Voice flows freely. The organization learns. Issues surface early.
Paternalism (Safe + Not worth it, upper-left): Compliance speech without commitment. People raise issues but doubt action.
Exploitation (Not safe + Worth it, lower-right): Selective disclosure. People speak only to trusted parties, often informally.
Exclusion (Not safe + Not worth it, lower-left): Silence. The organization is blind. Risk accumulates.
The leader's task is to move the team toward the upper-right quadrant: safe to speak, and worth speaking because action follows. Notice that psychological safety alone (upper row) is insufficient. If people feel safe but believe nothing will change, you get compliance speech: issues raised to check a box, without genuine expectation of response. This is the pattern that produces incident-reporting systems full of data that no one acts on.
Notice also that efficacy alone (left column) is insufficient. If people believe action is possible but do not feel safe raising the issue publicly, you get selective disclosure: the real concerns travel through trusted informal channels, bypassing the formal structures that could address them systematically.
The lower-right quadrant—neither safe nor worth it—produces organizational silence. Risk accumulates invisibly until something breaks. This is where sentinel events live before they surface.
Why This Matters in Healthcare Specifically
In most professional settings, the cost of speak-up failure is measured in suboptimal decisions, missed innovations, or eroded morale. In healthcare, the cost is measured differently. Patient safety is a function of the team's ability to surface near-misses before they become incidents, to challenge a wrong-site procedure plan before the incision is made, to flag the medication dosage that does not match the patient's weight, to interrupt the senior colleague whose decision is heading toward harm.
The empirical pattern is reliable. Sentinel events, never events, retained foreign objects, wrong-site surgeries, and many adverse drug events are traceable, after the fact, to a moment when someone on the team saw what was about to go wrong and could not bring it forward. The barrier was almost never knowledge. The barrier was almost always cultural. The team had learned, through prior experience, that speaking up in this environment carried a cost they were not willing to pay.
Speak-up culture is therefore not a workforce-engagement initiative dressed up in patient-safety language. It is patient-safety infrastructure. It is the mechanism by which the team's collective intelligence reaches the decision before harm occurs.
The Four Stages of Psychological Safety
Timothy Clark's framework identifies four sequential stages that teams move through as psychological safety develops. Each stage represents a threshold the leader must help the team cross.
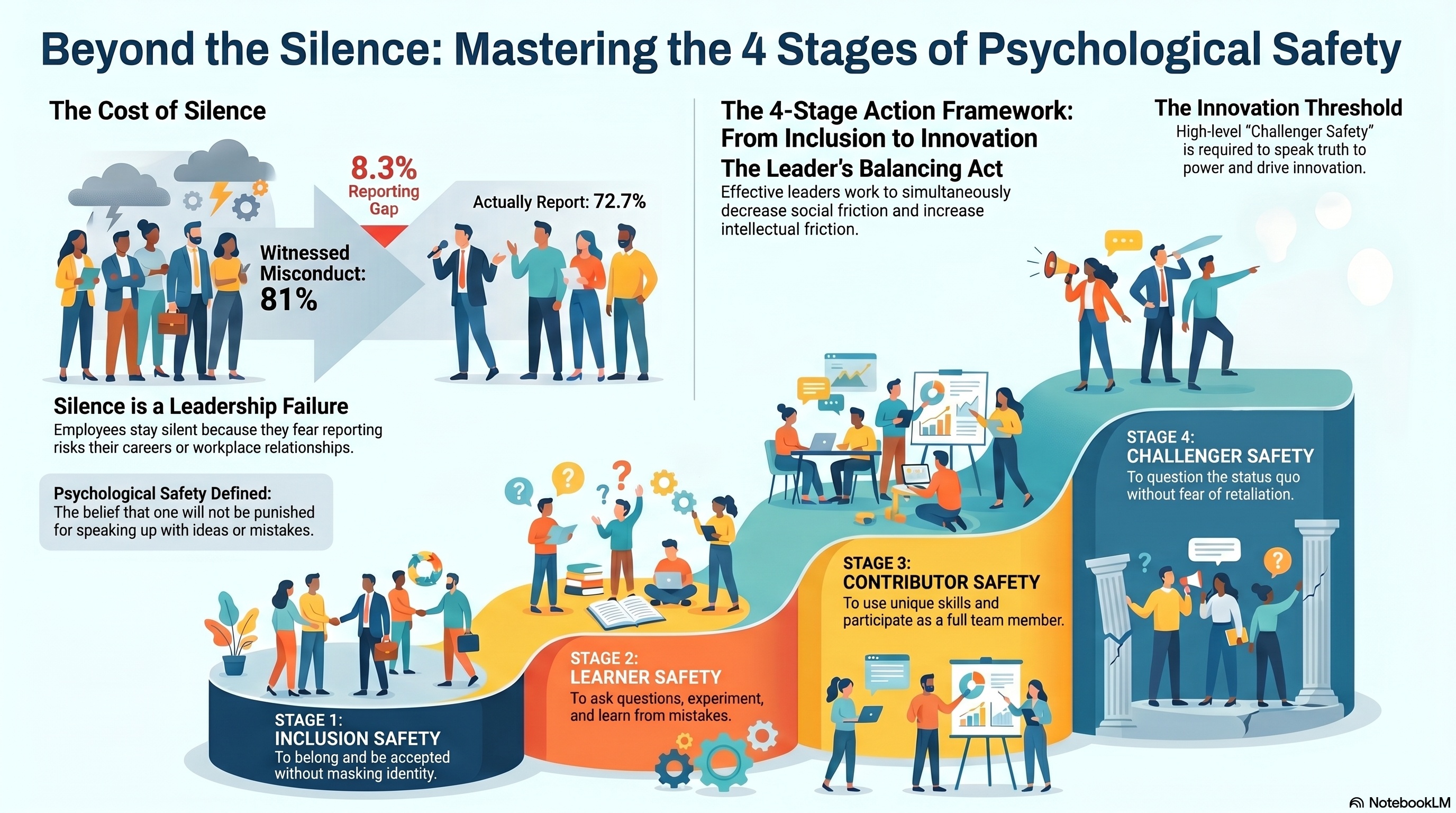
Stage 1: Inclusion Safety. The team member feels safe to belong and be accepted without masking identity. This is the foundation. Without inclusion safety, nothing else can be built.
Stage 2: Learner Safety. The team member feels safe to ask questions, experiment, and learn from mistakes. This is where curiosity survives contact with hierarchy.
Stage 3: Contributor Safety. The team member feels safe to use their unique skills and participate as a full team member. This is where diverse expertise actually reaches the work.
Stage 4: Challenger Safety. The team member feels safe to question the status quo without fear of retaliation. This is the innovation threshold, where speaking truth to power becomes possible.
The progression is not automatic. Each stage requires deliberate leader behavior, and each stage can be destroyed by a single punitive response. A team can have inclusion safety and learner safety but still lack challenger safety, which means junior members feel welcome and can ask questions but still will not challenge a senior colleague's decision when it matters most.
The Leader's Balancing Act: Intellectual vs. Social Friction
The leader's essential task is to simultaneously increase intellectual friction while decreasing social friction. Balancing these two forces is what allows a psychologically safe and innovative team to thrive.
High intellectual friction refers to task or process conflict. This is the productive, healthy tension that occurs when team members debate ideas, explore different perspectives, and rigorously question how things are done. In environments with high intellectual friction, teams achieve what Clark calls "Challenger Safety"—individuals feel confident speaking truth to power and challenging the status quo because they know it is necessary for the team to succeed. This type of friction is necessary for organizations to innovate, adapt to their environments, and catch potential errors before they develop into costly mistakes.
Low social friction refers to the absence of relationship conflict. An environment with low social friction is built on mutual respect and trust, meaning people do not feel interpersonal threat, fear of embarrassment, or worry over retaliation. The presence of fear in a team is a sign of weak leadership. When team members spend their time competing with or comparing themselves to one another, they lose the ability to genuinely connect.
The relationship between the two is highly interdependent: you cannot have high intellectual friction without low social friction. If social friction is high, employees will be too preoccupied with the risks of damaging workplace relationships or their own reputations to share their unique knowledge. They will remain silent to protect themselves. However, by intentionally driving down social friction, leaders eliminate the fear of punishment or marginalization. This creates the psychological safety necessary for employees to comfortably engage in the rigorous intellectual friction that actually drives a team's learning and success.
How It Connects to the Four Components
Speak-up culture is primarily a function of Components 1 and 2 of compassionate leadership, with downstream effects on Component 4.
Component 1: Notice. Speak-up is the mechanism by which the team supplements the leader's personal observation. Without speak-up, the leader is limited to what they can see directly, which is structurally inadequate at any meaningful scale.
Component 2: Interpret. Speak-up survives only when the team's reports are met with generous interpretation. Punitive interpretation kills speak-up faster than any policy can repair.
Component 4: Act. What the leader does with what was brought forward determines whether the team will bring forward the next thing. Action that addresses cause reinforces speak-up; action that punishes the messenger destroys it.
What It Looks Like in Practice
The leader thanks reporters before fixing the report. Whether the report is correct, partial, or mistaken, the act of bringing it forward is acknowledged before the substance is addressed.
Disagreement is invited, not tolerated. The leader actively asks for dissenting views in clinical decisions, and treats the views as valuable when they arrive.
Junior voices are amplified. In team meetings, the leader explicitly invites the most junior person to speak first on a question, before the seniority gradient compresses the conversation.
Reports of error are decoupled from punishment. Honest reporting of one's own error is met with calibrated response, not with reflexive consequence.
The leader names their own errors out loud. Modeling the behavior the leader wants from others is the strongest single signal in the room. A leader who never admits an error is implicitly telling the team that errors are not safe to admit.
What Speak-Up Culture Does Not Mean
Speak-up culture does not mean the abandonment of clinical hierarchy. The attending physician still has to make the call when the call is theirs to make. The clinical lead still has to set the standard. What changes is what happens before the call is made. Speak-up culture means that when the resident sees something the attending has missed, the resident says so, and the attending receives it as a contribution rather than as insubordination.
It also does not mean every voice is given equal weight. Calibrated speak-up culture distinguishes between novice observation and expert judgment, but does not silence either. The team learns that bringing forward what one has seen is always welcome; the eventual decision still belongs to the person whose role and expertise places it there.
The Evidence
Edmondson's foundational 1999 paper on psychological safety in work teams established the empirical anchor; her 2018 The Fearless Organization extends the framework into systematic guidance for leaders. Healthcare-specific applications include studies on operating-room speak-up (anesthesia and surgical teams), nursing-led interruption of error pathways, and the Joint Commission's body of root-cause analysis on sentinel events. The Joint Commission's repeated finding across decades is that communication failure is the most common contributing factor to sentinel events, and that the failure is reliably traceable to the team's prior experience of speaking up.
Sharp HealthCare's compassionate-culture transformation work, the Stanford CCARE evidence base, and the Worline and Dutton CompassionLab body of work each provide convergent evidence: speak-up cultures are produced by deliberate leader behavior and protected by deliberate organizational structure. They do not arise spontaneously, and they degrade quickly when neglected.
Diagnostic Questions
1. In the last month, has anyone on my team brought me bad news, dissent, or an error report unprompted? If not, what does that tell me?
2. When a team member reported an error or near-miss, what was the first thing I did? Did I thank them before I fixed it?
3. Do I model speak-up by naming my own errors out loud, or do I only ask others to name theirs?
4. In the last clinical decision I made that involved disagreement, did the most junior voice in the room get heard?
5. If a resident or new team member saw me about to make a wrong call this afternoon, would they say so? How do I actually know?
Care differently, not less.
References
- Edmondson, A. (1999). Psychological safety and learning behavior in work teams. Administrative Science Quarterly, 44(2), 350-383.
- Edmondson, A. C. (2018). The fearless organization: Creating psychological safety in the workplace for learning, innovation, and growth. Wiley.
- Sledjeski, S. (2023). The speak-up diagnostic: Is it safe? Is it worth it? Healthcare Leadership Review.
- The Joint Commission. (2024). Sentinel event data summary. The Joint Commission.
- Worline, M. C., & Dutton, J. E. (2017). Awakening compassion at work: The quiet power that elevates people and organizations. Berrett-Koehler.
Continue Reading
Why Your Last Wellness Program Failed
Most organizations have run compassion programs. Few have built cultivation systems. Six elements separate the two.
Compassion Culture and Patient Safety Are the Same Culture
Patient safety and staff well-being are not parallel investments. They are the same cultural fabric.